
湿疹(专业版)
湿疹,又称为特应性皮炎,是由多种因素引起的、常见的慢性皮肤炎症。其主要特点是皮肤发红、发痒,且易周期性地反复发作等,可能伴有哮喘或花粉热。
英文名称:Eczema,Atopic Dermatitis
定义
湿疹,又称为特应性皮炎,是由多种因素引起的、常见的慢性皮肤炎症。其主要特点是皮肤发红、发痒,且易周期性地反复发作等,可能伴有哮喘或花粉热。特应性皮炎没有治愈方法,但一些治疗和自我护理可以缓解症状、降低复发。病因
湿疹的确切原因仍未阐明,可能与消化系统疾病、精神紧张、失眠、过度疲劳、情绪变化、内分泌失调和代谢障碍等有关。遗传因素、生活环境、气候变化和致敏食物等也可导致湿疹发生。一般人群患病率为3-5%, 儿童可达10-20%。风险因素
增加湿疹几率的风险因素,包括如下:- 哮喘、花粉热
- 过敏
- 家族有湿疹或过敏性疾病史
- 生活在市区或低湿度的地方
- 接触某些织物,以及香水、肥皂、尘螨或食物等
- 精神压力
- 频繁清洗受影响的地方
- 皮肤抓痒
- 免疫抑制剂
- 超重或肥胖
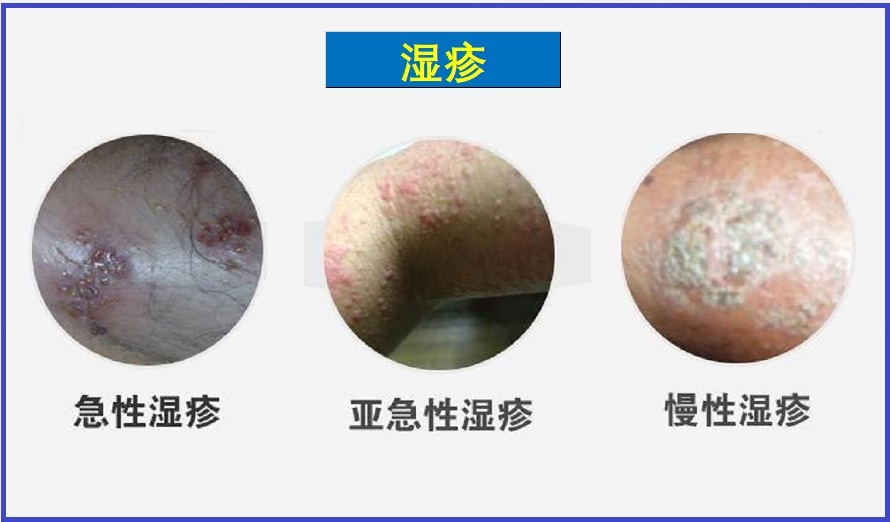
症状
症状因人而异。抓挠和摩擦会导致或加重某些症状。症状包括如下:
- 皮肤干燥、发痒
- 红色皮疹,在面颊、手臂和腿
- 红色、鳞屑
- 厚、革质的皮肤
- 皮肤上隆起的小疙瘩
- 结痂、渗出、或破裂的皮肤
- 症状恶化,冬天由于集中供热、室内空气干燥。
并发症
特应性皮炎(湿疹)的并发症可能包括:- 哮喘和花粉症:超过50%特应性皮炎幼儿患者在13岁时会患上哮喘和花粉症。
- 慢性瘙痒、鳞屑状皮肤。
- 皮肤感染。
- 过敏性接触性皮炎,在患有特应性皮炎的人中很常见。
- 睡眠问题,发作期可导致睡眠质量差。
疗法
湿疹治疗的主要目标是:- 治愈皮肤和保持健康
- 停止抓痒
- 避免皮肤感染
- 防止发作
- 识别和避免触发物
调整饮食与生活方式
- 经常吃酸奶,有助于调节肠道免疫、缓解瘙痒症状。
- 饮食富含深海鱼油、坚果,可减少湿疹皮炎。
- 避免引起过敏的食物。
- 经常运动锻炼,改善体质
- 学会和运用压力管理
营养与草本综合干预
以下是基于循证医学和循证营养学有关文献综合的结果。
有助于防控湿疹的营养和草本补充剂,主要包括如下:
1.维生素D:
充足的维生素D水平对许多皮肤状况是重要的,包括湿疹1,2。观察性研究数据的荟萃分析表明,特应性皮炎患者的血液维生素D水平低于健康皮肤患者3,4。另一项系统综述和荟萃分析包括四项观察性调查的结果,指出妊娠期维生素D水平较低的母亲所生的孩子患湿疹的风险较高5。
一项对65名受湿疹影响的参与者进行的安慰剂对照试验,使用每天125mcg(5000IU)的维生素D剂量与标准疗法联合治疗12周,发现那些血液中维生素D水平达到20ng/mL (50 nmol/L)或更高的人症状评分有所改善6。另一项对24名受试者进行的安慰剂对照试验发现,连续四周每天50mcg(2000IU)维生素D不仅改善了湿疹症状评分,而且减少了金黄色葡萄球菌的皮肤定植,一种与皮肤屏障功能障碍相关的细菌7。对四项随机安慰剂对照试验数据的荟萃分析发现,每天补充25mcg(1000IU)或40mcg(1600IU)的维生素D,持续1-2个月,可以有效降低湿疹症状的严重程度评分4。最近的一项荟萃分析也有类似的发现3。
2.γ-亚麻酸:
γ-亚麻酸(GLA)是一种具有抗炎作用的ω-6脂肪酸,一些证据表明,特应性皮炎患者缺乏将亚油酸(一种常见的植物来源的ω-6脂肪酸和一种必需营养素)转化为GLA所需的酶8,9。琉璃苣油、月见草油、黑加仑籽油和沙棘果油所含GLA特别丰富10。一项针对50名湿疹患者的随机对照试验发现,月见草油的剂量为每天1800 mg或3600 mg(分别提供160 mg或320 mg的GLA)(取决于年龄),4个月后比服用相同剂量的豆油更能改善湿疹症状11。在另一项对130名患有干性皮肤或轻度至中度特应性皮炎的成年受试者的对照试验中,每天富含200mg GLA持续12周的饮食比富含大豆/菜籽油混合物的饮食更能改善皮肤水合作用和减少皮肤炎症12。一项包括50名特应性皮炎患者的试验发现,根据年龄的不同,每天摄入500–6000mg月见草油,在减少湿疹症状和改善临床特征方面,持续五个月比葵花油更有效。对孕妇和婴儿的其他研究表明,补充GLA可以延缓儿童湿疹的发作并降低其严重程度13,14。
3.神经酰胺:
皮肤屏障功能障碍是皮炎的关键组成部分。皮肤中神经酰胺浓度的变化会导致皮肤屏障功能受损。因此,神经酰胺越来越多地用于局部制剂,以保护皮肤的完整性并改善皮肤水合作用。
神经酰胺也可以配制成口服制剂。这些配方可能含有来源于各种植物来源的神经酰胺,如小麦和魔芋。口服神经酰胺已被提议用于皮肤病,如皮炎和湿疹。几种动物模型表明,口服植物或细菌来源的神经酰胺可提高角质层含水量,减少经表皮水分损失,抑制炎性细胞因子(如白细胞介素-1β和IL-6)的表达,并改善皮肤弹性和恢复15-17。
临床研究表明,口服植物来源的神经酰胺也能改善皮肤健康的几个方面。在一项临床研究中,特应性皮炎儿童每天服用1.8mg魔芋衍生神经酰胺或安慰剂,为期两周。到研究结束时,治疗组的25名儿童的皮肤症状和过敏反应有所改善,但安慰剂组的25例儿童没有改善18。与安慰剂相比,相同剂量的神经酰胺在8-12周后可减少42名健康成年人的经表皮水分损失19。在14名20-54岁患有轻度至中度特应性湿疹的成年参与者中,与基线相比,每天1.8mg魔芋神经酰胺可在2-8周后减少经表皮水分损失20。在一项临床研究中,51名参与者随机接受安慰剂或每天5mg魔芋提取物神经酰胺,摄入神经酰胺可显著降低皮肤干燥、发红和瘙痒21。来自小麦的神经酰胺也被证明可以改善皮肤健康:一项安慰剂对照试验招募了51名20-63岁的干性皮肤女性,发现与安慰剂相比,350mg富含神经酰胺的小麦提取物油在使用三个月后改善了皮肤水合作用22。
4.维生素E:
维生素E是一种脂溶性营养素,可以降低氧化应激,保护体内的脂肪化合物免受自由基损伤。长期以来,人们都知道它在皮肤健康中起着重要作用,在患有各种炎症性皮肤问题(包括特应性皮炎)的人身上也观察到了低水平的维生素E23,24。
在一项针对70名特应性皮肤炎受试者的随机安慰剂对照试验中,在四个月内每天400IU的维生素E(未指定形式)可以减轻湿疹症状25。一项针对45名参与者的安慰剂对照试验发现,每天600IU的dl-α-生育酚(相当于约300 IU的活性d-α-生育醇)和每天40mcg(1600IU)的维生素D3都比安慰剂更能减轻湿疹症状,但维生素E和维生素D的治疗效果更大26。另一项试验包括96名患有特应性皮炎的受试者,并将每天服用400 IU d- α -生育酚的治疗与安慰剂进行比较。8个月后,50名服用维生素e的参与者中有30人(60%)出现了显著改善或接近完全缓解,而46名服用安慰剂的参与者中只有1人(2%)出现了改善27。
局部维生素E经常被推荐作为特应性皮炎治疗的一部分28。在一项为期28天的临床试验中,含有维生素E以及绿茶儿茶素(EGCG)和葡萄籽原花青素的乳膏比安慰剂乳膏更能改善皮肤症状,该试验包括44名面部和/或颈部特应性皮肤炎参与者29。尽管它是安全的,但仍有罕见的因局部维生素E过敏反应而引起的接触性皮炎病例报告30。
5.益生菌:
大量临床试验表明,口服益生菌补充剂可以降低湿疹的风险和严重程度。对随机对照试验的全面审查发现,某些益生菌在怀孕期间服用或在婴儿期或儿童期服用,可以有效预防和治疗特应性皮炎。通常使用乳酸菌与双歧杆菌组合,已经证明了最佳效果31-33。副干酪乳杆菌、鼠李糖乳杆菌、嗜酸乳杆菌、鼠李糖乳杆菌GG、干酪乳杆菌,唾液乳杆菌、植物乳杆菌、长双歧杆菌、动物乳杆菌亚种和双歧杆菌的益生菌菌株,以不同的组合使用,每天提供总计10亿CFU或更多,被发现对特应性皮炎有积极作用31,32。
6.乳清蛋白:
乳清蛋白来自牛奶,与酪蛋白(主要的牛奶蛋白)的不同之处在于其组成,包括乳球蛋白、免疫球蛋白、牛白蛋白和乳铁蛋白组成34。由乳清蛋白部分水解产生的小肽被认为可以刺激平衡的免疫激活,从而增强免疫耐受性35。
一项对8项随机对照试验结果的荟萃分析发现,对于因家族史而有过敏和湿疹高风险的婴儿,用部分水解的乳清婴儿配方奶粉代替或补充母乳,与牛奶配方奶粉相比,可以降低患湿疹的风险36。对八项临床试验的回顾结果进一步表明,部分水解乳清配方奶粉不仅可以降低高危婴儿患特应性皮炎的风险,而且可以降低普通婴儿患特异性皮炎的风险,同时支持正常的生长发育37。一项双盲随机对照临床试验表明,与安慰剂相比,口服补充乳清蛋白似乎可以改善接触性皮炎(CD)的症状38。动物研究表明,部分水解乳清配方奶粉可以改善皮肤屏障功能39。这可能是其对湿疹有益的部分原因。
需要注意的是,部分水解乳清配方奶粉不适合已知有牛奶过敏性的婴儿40。
7.褪黑素:
睡眠障碍在特应性皮炎患者中很常见,虽然强烈的瘙痒是一个明显的因素,但有证据表明,它并不能完全解释这种关系41,42。睡眠不足会降低生活质量,并引发压力反应,甚至可能导致湿疹恶化,从而导致恶性循环43。褪黑素是一种在大脑和皮肤细胞中产生的激素,被认为在皮肤炎中起作用44。褪黑素不仅调节昼夜节律,如睡眠和觉醒周期,还可以减少皮肤氧化应激和炎症,保护皮肤免受太阳辐射损伤,并似乎可以促进伤口愈合和皮肤屏障健康41,42,44。
一项观察性研究指出,在36名患有特应性皮炎的成年人中,褪黑素水平较低与湿疹更严重、瘙痒更剧烈和睡眠更差有关45。一项随机对照试验调查了70名6-12岁湿疹儿童每晚服用6mg褪黑激素的效果。六周后,与服用安慰剂的儿童相比,服用褪黑素的儿童在症状严重程度指数和睡眠习惯问卷方面的得分有了更大的改善,尽管没有记录到瘙痒、入睡时间或总睡眠时间的改善。此外,褪黑激素降低了IgE水平,IgE是一种与特应性皮炎和其他过敏性疾病有关的抗体类型46。在一项针对48名1-18岁特应性皮肤炎儿童的交叉试验中,在降低湿疹症状评分和缩短入睡时间方面,每晚3mg、持续四周的褪黑激素比安慰剂更有效47。
局部褪黑素可能比口服褪黑素有优势,因为它提高了皮肤褪黑素的浓度,同时绕过了消化道中的代谢44。一项使用特应性皮炎小鼠模型的研究表明,局部褪黑素也可能产生有益的效果48。
8.欧米伽3脂肪酸:
Omega-3脂肪酸,如鱼油中的EPA和DHA,具有众所周知的抗炎作用。一些研究表明,在怀孕和哺乳期间摄入更多的这些脂肪酸与婴儿和儿童湿疹及其他过敏性疾病的风险较低有关,但并非所有研究结果都一致49,50。同样,大多数但并非所有的研究都注意到,婴儿和儿童时期摄入更多的鱼与过敏性疾病(包括特应性皮肤炎)的发病率较低之间存在相关性51。
在一项包括53名成人特应性皮炎患者的对照试验中,与饱和脂肪安慰剂相比,每天5.4g DHA治疗8周可使湿疹症状评分降低52。一项包括31名特应性皮炎患者的试验发现,服用鱼油的受试者在12周后,鳞屑、瘙痒和总体严重程度都有了更大的减轻;受试者每天服用10g(约2茶匙)鱼油,提供1.8g EPA,或服用含有橄榄油的安慰剂53。在另一项针对22名中重度湿疹患者的试验中,每天用200ml 10%鱼油乳液或10%大豆油(富含ω-6脂肪酸、亚麻酸)乳液静脉注射10天,可以改善湿疹症状,但静脉注射鱼油的效果更大54。
9.锌:
锌是正常皮肤功能和修复所必需的,据报道,锌缺乏在特应性皮肤炎患者中更为常见55。然而,很少有临床试验检测锌用于治疗湿疹。一项针对58名头发锌水平较低的2至14岁湿疹儿童的对照试验发现,在八周内每天12mg锌(以氧化锌形式)可以减少瘙痒并改善皮肤水分56。然而,每天185.4mg(相当于约43mg元素锌)的硫酸锌,在一项为期八周的安慰剂对照试验中,对50名1-16岁患有特应性皮炎和锌状况不明的儿童的症状严重程度没有改善57,这表明适当的剂量和患者选择可能是获得良好结果的关键。
局部锌也可能在治疗特应性皮炎中发挥作用。在一项不受控制的临床试验中,一种含有抗炎草药提取物和淀粉的氧化锌霜被用于治疗30名患有轻度至中度特应性皮炎的儿童,该皮炎影响面部、手臂或躯干。六周后,87%的儿童湿疹症状严重程度评分改善了50%以上58。一项有趣的研究发现,连续三个晚上穿着氧化锌浸渍材料制成的衣服睡觉,可以减轻症状的严重程度和瘙痒,并改善特应性皮肤炎患者的睡眠59。
10.蜂蜜:
蜂蜜是一种主要由果糖和葡萄糖组成的复杂物质,但有的也富含黄酮类化合物、有机酸和其他植物化学物质,其中一些具有强大的抗炎、氧化应激降低和抗菌能力60。在一项不受控制的试点试验中,16名有两个或两个以上类似病变的特应性皮炎患者连续7个晚上每晚使用纯麦卢卡蜂蜜涂抹在他们的一些病变上,用纱布覆盖,并在早上洗掉。两名患者的皮肤症状在两个晚上内恶化,并停止蜂蜜治疗;然而,在剩下的14名参与者中,经治疗的病变有所改善,而未经治疗的则没有。此外,14名患者中有3人(21%)在一年后报告病情持续好转61。一项研究发现,在10名未经治疗的特应性皮炎患者中,有8人(80%)的症状得到了显著改善。在同一项研究中,11名接受局部皮质类固醇治疗的特应性皮炎患者使用不同比例的皮质类固醇加蜂蜜/蜂蜡/橄榄油混合物代替了这种治疗。即使在使用了比研究开始时少75%皮质类固醇的配方制剂后,11人中有5人(45%)的症状也没有恶化62。
11.姜黄素:
姜黄素具有众所周知的抗炎作用。临床前证据表明,口服和外用姜黄素都可能在治疗皮肤疾病中发挥作用,包括特应性和接触性(或刺激性)皮炎63,64。在一项包括42名接受标准局部护理的特应性皮炎患者的公开临床试验中,与仅使用标准治疗措施的人相比,每天两次服用500mg姜黄素植物体(一种生物可利用的姜黄素形式)的患者皮肤水合作用和弹性更好,症状严重程度更低65。据报道,一种由包括姜黄在内的六种草药提取物制成的乳膏在150名特应性皮炎患者4周后减轻了湿疹症状66。在一项有96名参与者的安慰剂对照试验中,每天1000mg姜黄素,持续四周,可减轻因暴露于有毒芥末而患慢性皮炎的男性的瘙痒,提高生活质量67。对小鼠的研究表明,姜黄素可抑制特应性皮炎引起的炎症反应,降低患进行性过敏性疾病的风险68,69。
12.槲皮素:
槲皮素是饮食中最丰富的黄酮类化合物之一,已被证明可以抑制炎症信号传导和减少组胺释放。大量实验室和动物研究表明,槲皮素可能帮助治疗特应性皮炎70,71。在10名镍过敏志愿者中,每天服用2000mg槲皮素,持续三天,可减少他们的镍反应:8名受试者的镍反应减少了50%,2名受试人的镍反应降低了100%72。此外,在光照前两小时服用1000mg槲皮素,据报道,在一项针对9名受试者的研究中,可以减少光敏性皮炎(一种对阳光照射的湿疹样反应)72。
13.维生素C:
维生素C是一种水溶性自由基清除剂,高度集中在皮肤最外层73。维生素C在维持皮肤屏障方面具有重要作用,一些证据表明它具有抗组胺和抗过敏作用73-75。研究发现,受特应性皮炎影响的皮肤的维生素C浓度低于健康皮肤76。
一项针对17名患有特应性皮肤炎的成年人的研究发现,血液中维生素C水平的降低与皮肤神经酰胺(一种保护性脂质)水平的降低和湿疹症状的严重程度的增加有关77。一项包括65名有过敏史的女性的研究发现,富含维生素C的饮食会增加母乳中的维生素C水平,并与其后代在出生第一年患特应性皮炎的发病率较低有关;然而,补充维生素C对婴儿的母乳水平或特应性皮炎风险没有影响78。尽管维生素C不易被皮肤吸收,但在特应性皮肤炎小鼠模型中,发现含有氧化锌基维生素C的局部乳膏可以减少皮肤炎症79。
14.维生素A和类胡萝卜素:
维生素A是一种脂溶性必需营养素,用于免疫功能、健康的粘膜(如肠道和呼吸系统的衬里)和上皮(如皮肤)屏障功能。维生素A缺乏与皮肤炎症、伤口愈合不良、皮肤微生物组破坏和皮肤感染风险增加有关80。胡萝卜素是维生素A的前体,与被称为类胡萝卜素的相关化合物一起,具有独特的免疫调节和抗氧化作用。观察证据表明,特应性皮炎患者的维生素A代谢异常,皮肤和血液中的维生素A水平较低,血液中的类胡萝卜素叶黄素和玉米黄原水平较低81,82。对特应性皮肤炎动物模型的研究表明,β-胡萝卜素和类胡萝卜素虾青素可能具有抗湿疹作用83,84。
15.沙棘油:
沙棘油富含黄酮类化合物、类胡萝卜素、多不饱和脂肪酸(如GLA)和其他植物化学物质,历来被用于治疗皮炎和其他皮肤疾病。临床前证据表明,沙棘油可能具有抗菌、抗炎和伤口愈合作用85。一项实验室研究表明,沙棘籽油可以逆转金黄色葡萄球菌对皮肤细胞功能的负面影响86,和几项动物研究表明,它可以减少湿疹87,88。一项针对49名特应性皮炎患者的临床试验发现,每天服用5g沙棘果肉提取的油,持续四个月,可以显著改善症状89。
更多内容可点击其个性化综合干预方案如下:
以及参阅本网如下专文了解更多有关内容:
医疗干预
常规治疗包括如下:
- 药物治疗可包括如下:
- 处方药膏和含有可的松、他克莫司软膏,或吡美莫司
- 非处方或处方抗组胺药,有助于防止瘙痒
- 抗生素直接应用于皮肤或口服,以治疗感染
- 口服药物,如强的松或环孢菌素,对严重病例
- 杜伐布单抗注射,用于减轻严重情况下的肿胀
- 光疗法:如果皮肤护理和药物治疗无效,可以使用光疗:
- 紫外线A光和5-甲氧基补骨脂素(PUVA)
- 光分离置换法,适用于严重病例。
家庭护理
适当的皮肤护理可以让皮肤愈合,如:
- 避免热的、长时间的淋浴,不要超过15分钟。
- 使用温和的、无味的肥皂或无皂清洁剂,或尽量少用。
- 沐浴后轻轻拍干、吹干燥身体。当皮肤仍然潮湿时,涂上温和的润肤霜。
- 要及时治疗皮肤感染。
预防
湿疹无法预防,但一些措施可以降低发作如:- 每天至少两次保湿,使用无刺激的软膏、霜剂和乳液等保湿剂。婴幼儿可以使用凡士林预防特应性皮炎。
- 识别并避免使症状恶化的触发因素,包括精神压力、汗液、刺激性肥皂、洗涤剂、灰尘和花粉等。·
- 避免过敏食物,如牛奶、花生、鸡蛋、大豆、贝壳类和海鲜...等。
- 限制淋浴时间,不要用太热的水,温水最佳。·
- 使用温和的肥皂,除臭和抗菌等刺激性肥皂不宜。
- 小心保养,沐浴后,用柔软的毛巾轻轻擦拭皮肤,并在皮肤潮湿时涂抹保湿霜。
参考文献:
1. Kechichian E, Ezzedine K. Vitamin D and the Skin: An Update for Dermatologists. American journal of clinical dermatology. Apr 2018;19(2):223-235
2. Mansour NO et al. The impact of vitamin D supplementation as an adjuvant therapy on clinical outcomes in patients with severe atopic dermatitis: A randomized controlled trial. Pharmacology research & perspectives. Dec 2020;8(6):e00679.
3. Ng JC, Yew YW. Effect of Vitamin D Serum Levels and Supplementation on Atopic Dermatitis: A Systematic Review and Meta-analysis. American journal of clinical dermatology. 2022 May;23(3):267-275.
4. Kim MJ et al. Vitamin D Status and Efficacy of Vitamin D Supplementation in Atopic Dermatitis: A Systematic Review and Meta-Analysis. Nutrients. Dec 3 2016;8(12)
5. Wei Z et al. Maternal vitamin D status and childhood asthma, wheeze, and eczema: A systematic review and meta-analysis. Pediatr Allergy Immunol. Sep 2016;27(6):612-9.
6. Sanchez-Armendariz K et al. Oral vitamin D3 5000 IU/day as an adjuvant in the treatment of atopic dermatitis: a randomized control trial. Int J Dermatol. Dec 2018;57(12):1516-1520.
7. Udompataikul M et al. The Effects of Oral Vitamin D Supplement on Atopic Dermatitis: A Clinical Trial with Staphylococcus aureus Colonization Determination. Journal of the Medical Association of Thailand. Oct 2015;98 Suppl 9:S23-30.
8. Horrobin DF. Fatty acid metabolism in health and disease: the role of delta-6-desaturase. Am J Clin Nutr. May 1993;57(5 Suppl):732S-736S; discussion 736S-737S.
9. Yen CH et al. Linoleic acid metabolite levels and transepidermal water loss in children with atopic dermatitis. Ann Allergy Asthma Immunol. Jan 2008;100(1):66-73.
10. Zielińska A et al. Abundance of active ingredients in sea-buckthorn oil. Lipids in health and disease. May 19 2017;16(1):95.
11. Chung BY et al. Effect of Evening Primrose Oil on Korean Patients With Mild Atopic Dermatitis: A Randomized, Double-Blinded, Placebo-Controlled Clinical Study. Annals of dermatology. Aug 2018;30(4):409-416.
12. Senapati S et al. Evening primrose oil is effective in atopic dermatitis: a randomized placebo-controlled trial. Indian journal of dermatology, venereology and leprology. Sep-Oct 2008;74(5):447-52.
13. van Gool CJ et al. Gamma-linolenic acid supplementation for prophylaxis of atopic dermatitis--a randomized controlled trial in infants at high familial risk. Am J Clin Nutr. Apr 2003;77(4):943-51.
14. Linnamaa P et al. Blackcurrant seed oil for prevention of atopic dermatitis in newborns: a randomized, double-blind, placebo-controlled trial. Clin Exp Allergy. Aug 2010;40(8):1247-55.
15. Tokudome Y. Influence of Oral Administration of Lactic Acid Bacteria Metabolites on Skin Barrier Function and Water Content in a Murine Model of Atopic Dermatitis. Nutrients. 2018 Dec 1;10(12):1858.
16. Yeom M et al. Oral administration of glucosylceramide ameliorates inflammatory dry-skin condition in chronic oxazolone-induced irritant contact dermatitis in the mouse ear. J Dermatol Sci. Aug 2012;67(2):101-10.
17. Tsuji K et al. Dietary glucosylceramide improves skin barrier function in hairless mice. J Dermatol Sci. Nov 2006;44(2):101-7.
18. Kimata H. Improvement of atopic dermatitis and reduction of skin allergic responses by oral intake of konjac ceramide. Pediatric dermatology. Jul-Aug 2006;23(4):386-9.
19. Uchiyama T et al. Oral Intake of Glucosylceramide Improves Relatively Higher Level of Transepidermal Water Loss in Mice and Healthy Human Subjects. Journal of Health Science. 2008;54(5):559-566.
20. Miyanishi K et al. Reduction of transepidermal water loss by oral intake of glucosylceramides in patients with atopic eczema. Allergy. 2005 Nov;60(11):1454-5.
21. Heggar Venkataramana S et al. Potential benefits of oral administration of AMORPHOPHALLUS KONJAC glycosylceramides on skin health - a randomized clinical study. BMC Complement Med Ther. Jan 31 2020;20(1):26.
22. Guillou S et al. The moisturizing effect of a wheat extract food supplement on women's skin: a randomized, double-blind placebo-controlled trial. Int J Cosmet Sci. Apr 2011;33(2):138-43.
23. Liu X et al. Serum vitamin E levels and chronic inflammatory skin diseases: A systematic review and meta-analysis. PLoS One. 2021;16(12):e0261259.
24. Berardesca E et al. Vitamin E supplementation in inflammatory skin diseases. Dermatologic therapy. Nov 2021;34(6):e15160.
25. Jaffary F et al. Effects of oral vitamin E on treatment of atopic dermatitis: A randomized controlled trial. Journal of research in medical sciences. Nov 2015;20(11):1053-7.
26. Javanbakht MH et al. Randomized controlled trial using vitamins E and D supplementation in atopic dermatitis. The Journal of dermatological treatment. Jun 2011;22(3):144-50.
27. Tsoureli-Nikita E et al. Evaluation of dietary intake of vitamin E in the treatment of atopic dermatitis: a study of the clinical course and evaluation of the immunoglobulin E serum levels. Int J Dermatol. Mar 2002;41(3):146-50.
28. Panin G et al. Topical alpha-tocopherol acetate in the bulk phase: eight years of experience in skin treatment. Ann N Y Acad Sci. Dec 2004;1031:443-7.
29. Patrizi A et al. Randomized, controlled, double-blind clinical study evaluating the safety and efficacy of MD2011001 cream in mild-to-moderate atopic dermatitis of the face and neck in children, adolescents and adults. The Journal of dermatological treatment. Aug 2016;27(4):346-50.
30. Teo CWL et al. Vitamin E in Atopic Dermatitis: From Preclinical to Clinical Studies. Dermatology. 2021;237(4):553-564.
31. Tan-Lim CSC et al. Comparative effectiveness of probiotic strains on the prevention of pediatric atopic dermatitis: A systematic review and network meta-analysis. Pediatr Allergy Immunol. Aug 2021;32(6):1255-1270.
32. Jiang W et al. The Role of Probiotics in the Prevention and Treatment of Atopic Dermatitis in Children: An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials. Paediatr Drugs. Oct 2020;22(5):535-549.
33. Amalia N et al. Systematic review and meta-analysis on the use of probiotic supplementation in pregnant mother, breastfeeding mother and infant for the prevention of atopic dermatitis in children. The Australasian journal of dermatology. May 2020;61(2):e158-e173.
34. Cabana MD. The Role of Hydrolyzed Formula in Allergy Prevention. Ann Nutr Metab. 2017;70 Suppl 2:38-45.
35. Vandenplas Y et al. A perspective on partially hydrolyzed protein infant formula in nonexclusively breastfed infants. Korean journal of pediatrics. May 2019;62(5):149-154.
36. Szajewska H et al. A partially hydrolyzed 100% whey formula and the risk of eczema and any allergy: an updated meta-analysis. The World Allergy Organization journal. 2017;10(1):27.
37. Sauser J et al. Partially Hydrolyzed Whey Infant Formula: Literature Review on Effects on Growth and the Risk of Developing Atopic Dermatitis in Infants from the General Population. Int Arch Allergy Immunol. 2018;177(2):123-134.
38. Alyasin S et al. Efficacy of oral supplementation of whey protein in patients with contact dermatitis: A pilot randomized double-blind placebo-controlled clinical trial. Dermatologic therapy. Nov 2020;33(6):e14260.
39. Holvoet S et al. Partially Hydrolysed Whey-Based Infant Formula Improves Skin Barrier Function. Nutrients. Sep 4 2021;13(9)
40. Chung CS et al. FDA's health claim review: whey-protein partially hydrolyzed infant formula and atopic dermatitis. Pediatrics. Aug 2012;130(2):e408-14.
41. Jaworek AK et al. Melatonin as an Antioxidant and Immunomodulator in Atopic Dermatitis-A New Look on an Old Story: A Review. Antioxidants (Basel, Switzerland). Jul 24 2021;10(8)
42. Chang YS et al. Mechanism of Sleep Disturbance in Children with Atopic Dermatitis and the Role of the Circadian Rhythm and Melatonin. International journal of molecular sciences. Mar 29 2016;17(4):462.
43. Gupta MA et al. Sleep-wake disorders and dermatology. Clin Dermatol. Jan-Feb 2013;31(1):118-26.
44. Rusanova I et al. Protective Effects of Melatonin on the Skin: Future Perspectives. International journal of molecular sciences. 2019 Oct 8;20(19):4948.
45. Jaworek AK et al. Melatonin and sleep disorders in patients with severe atopic dermatitis. Postepy dermatologii i alergologii. Oct 2021;38(5):746-751.
46. Taghavi Ardakani A et al. The effects of melatonin administration on disease severity and sleep quality in children with atopic dermatitis: A randomized, double-blinded, placebo-controlled trial. Pediatr Allergy Immunol. Dec 2018;29(8):834-840.
47. Chang YS et al. Melatonin Supplementation for Children With Atopic Dermatitis and Sleep Disturbance: A Randomized Clinical Trial. JAMA pediatrics. Jan 2016;170(1):35-42.
48. Chang YS et al. Topical Melatonin Exerts Immunomodulatory Effect and Improves Dermatitis Severity in a Mouse Model of Atopic Dermatitis. International journal of molecular sciences. 2022 Jan 25;23(3):1373.
49. Miles EA et al. Can Early Omega-3 Fatty Acid Exposure Reduce Risk of Childhood Allergic Disease? Nutrients. 2017 Jul 21;9(7):784.
50. Best KP et al. Omega-3 long-chain PUFA intake during pregnancy and allergic disease outcomes in the offspring: a systematic review and meta-analysis of observational studies and randomized controlled trials. Am J Clin Nutr. Jan 2016;103(1):128-43.
51. Kremmyda LS et al. Atopy risk in infants and children in relation to early exposure to fish, oily fish, or long-chain omega-3 fatty acids: a systematic review. Clin Rev Allergy Immunol. Aug 2011;41(1):36-66.
52. Koch C et al. Docosahexaenoic acid (DHA) supplementation in atopic eczema: a randomized, double-blind, controlled trial. Br J Dermatol. Apr 2008;158(4):786-92.
53. Bjorneboe A et al. Effect of n-3 fatty acid supplement to patients with atopic dermatitis. J Intern Med Suppl. 1989;731:233-6.
54. Mayser P et al. A double-blind, randomized, placebo-controlled trial of n-3 versus n-6 fatty acid-based lipid infusion in atopic dermatitis. JPEN Journal of parenteral and enteral nutrition. May-Jun 2002;26(3):151-8.
55. Gray NA et al. Zinc and atopic dermatitis: a systematic review and meta-analysis. J Eur Acad Dermatol Venereol. Jun 2019;33(6):1042-1050.
56. Kim JE et al. Hair zinc levels and the efficacy of oral zinc supplementation in patients with atopic dermatitis. Acta dermato-venereologica. Sep 2014;94(5):558-62.
57. Ewing CI et al. Failure of oral zinc supplementation in atopic eczema. European journal of clinical nutrition. Oct 1991;45(10):507-10.
58. Licari A et al. A starch, glycyrretinic, zinc oxide and bisabolol based cream in the treatment of chronic mild-to-moderate atopic dermatitis in children: a three-center, assessor blinded trial. Minerva pediatrica. Dec 2017;69(6):470-475.
59. Wiegand C et al. Skin-protective effects of a zinc oxide-functionalized textile and its relevance for atopic dermatitis. Clin Cosmet Investig Dermatol. 2013;6:115-21. \
60. Aw Yong PY et al. The Potential use of Honey as a Remedy for Allergic Diseases: A Mini Review. Frontiers in pharmacology. 2020;11:599080.
61. Alangari AA et al. Honey is potentially effective in the treatment of atopic dermatitis: Clinical and mechanistic studies. Immun Inflamm Dis. Jun 2017;5(2):190-199.
62. Al-Waili NS. Topical application of natural honey, beeswax and olive oil mixture for atopic dermatitis or psoriasis: partially controlled, single-blinded study. Complementary therapies in medicine. Dec 2003;11(4):226-34.
63. Vaughn AR et al. Effects of Turmeric (Curcuma longa) on Skin Health: A Systematic Review of the Clinical Evidence. Phytother Res. Aug 2016;30(8):1243-64.
64. Vollono L et al. Potential of Curcumin in Skin Disorders. Nutrients. 2019 Sep 10;11(9):2169.
65. Togni S et al. Oral curcumin (Meriva®) reduces symptoms and recurrence rates in subjects with atopic dermatitis. Esperienze Dermatologiche. 2019;21(2-4):42-46.
66. Rawal RC et al. Clinical evaluation of an Indian polyherbal topical formulation in the management of eczema. Journal of alternative and complementary medicine (New York, NY). Jun 2009;15(6):669-72.
67. Panahi Y et al. Improvement of sulphur mustard-induced chronic pruritus, quality of life and antioxidant status by curcumin: results of a randomised, double-blind, placebo-controlled trial. The British journal of nutrition. Oct 2012;108(7):1272-9.
68. Shin HS et al. Turmeric (Curcuma longa) attenuates food allergy symptoms by regulating type 1/type 2 helper T cells (Th1/Th2) balance in a mouse model of food allergy. Journal of ethnopharmacology. Dec 4 2015;175:21-9.
69. Sharma S et al. Curcumin Ameliorates Ovalbumin-Induced Atopic Dermatitis and Blocks the Progression of Atopic March in Mice. Inflammation. Feb 2020;43(1):358-369.
70. Karuppagounder V et al. Molecular targets of quercetin with anti-inflammatory properties in atopic dermatitis. Drug discovery today. Apr 2016;21(4):632-9.
71. Jafarinia M et al. Quercetin with the potential effect on allergic diseases. Allergy, asthma, and clinical immunology. 2020;16:36.
72. Weng Z et al. Quercetin is more effective than cromolyn in blocking human mast cell cytokine release and inhibits contact dermatitis and photosensitivity in humans. PLoS One. 2012;7(3):e33805.
73. Wang K et al. Role of Vitamin C in Skin Diseases. Front Physiol. 2018;9:819.
74. Hagel AF et al. Intravenous infusion of ascorbic acid decreases serum histamine concentrations in patients with allergic and non-allergic diseases. Naunyn-Schmiedeberg's archives of pharmacology. Sep 2013;386(9):789-93.
75. Vollbracht C et al. Intravenous vitamin C in the treatment of allergies: an interim subgroup analysis of a long-term observational study. The Journal of international medical research. Sep 2018;46(9):3640-3655.
76. Leveque N et al. High iron and low ascorbic acid concentrations in the dermis of atopic dermatitis patients. Dermatology. 2003;207(3):261-4.
77. Shin J et al. Associations among plasma vitamin C, epidermal ceramide and clinical severity of atopic dermatitis. Nutrition research and practice. Aug 2016;10(4):398-403.
78. Hoppu U et al. Vitamin C in breast milk may reduce the risk of atopy in the infant. European journal of clinical nutrition. Jan 2005;59(1):123-8.
79. Lee JH et al. Effects of VitabridC(12) on Skin Inflammation. Annals of dermatology. Oct 2017;29(5):548-558.
80. Roche FC et al. Illuminating the Role of Vitamin A in Skin Innate Immunity and the Skin Microbiome: A Narrative Review. Nutrients. 2021 Jan 21;13(2):302.
81. Lucas R et al. Reduced Carotenoid and Retinoid Concentrations and Altered Lycopene Isomer Ratio in Plasma of Atopic Dermatitis Patients. Nutrients. 018 Oct 1;10(10):1390.
82. Mihaly J et al. Decreased retinoid concentration and retinoid signalling pathways in human atopic dermatitis. Experimental dermatology. Apr 2011;20(4):326-30.
83. Hiragun M et al. Oral administration of beta-carotene or lycopene prevents atopic dermatitis-like dermatitis in HR-1 mice. J Dermatol. Oct 2016;43(10):1188-1192.
84. Park JW et al. Effect of Astaxanthin on Anti-Inflammatory and Anti-Oxidative Effects of Astaxanthin Treatment for Atopic Dermatitis-induced Mice. Journal of Acupuncture Research. 2021;38(4):293-299.
85. Pundir S et al. Ethnomedicinal uses, phytochemistry and dermatological effects of Hippophae rhamnoides L.: A review. Journal of ethnopharmacology. Feb 10 2021;266:113434.
86. Shah H et al. Hippophae rhamnoides mediate gene expression profiles against keratinocytes infection of Staphylococcus aureus. Molecular biology reports. Feb 2021;48(2):1409-1422.
87. Wang X et al. Ameliorative effects of sea buckthorn oil on DNCB induced atopic dermatitis model mice via regulation the balance of Th1/Th2. BMC Complement Med Ther. Aug 26 2020;20(1):263.
88. Hou DD et al. Sea Buckthorn (Hippophae rhamnoides L.) Oil Improves Atopic Dermatitis-Like Skin Lesions via Inhibition of NF-kappaB and STAT1 Activation. Skin Pharmacol Physiol. 2017;30(5):268-276.
89. Yang B et al. Effects of dietary supplementation with sea buckthorn (Hippophae rhamnoides) seed and pulp oils on atopic dermatitis. J Nutr Biochem. Nov 1999;10(11):622-30.
参考来源:
美国梅奥诊所
www.mayoclinic.org
美国湿疹学会
http://www.eczema.org
美国过敏、哮喘和免疫学学会
http://www.aaaai.org
美国国立卫生研究院公众健康网
www.medlineplus.gov
加拿大皮肤科协会
http://www.dermatology.ca
免责声明和安全信息
- 本信息(包括任何附带资料)不是为了取代医生或有关合格从业人士的建议或忠告。
- 任何人如果想要对本文涉及的药物、饮食、运动或其他生活方式的使用、或改变调整,以预防或治疗某一特定健康状况或疾病,应首先咨询医生或有关合格从业人士,并获得他/她们的许可。妊娠和哺乳妇女在使用本网站任何内容前,尤其应征求医生的意见。
- 除非另有说明,本网站所述内容仅适用于成人。
- 本网站所推荐的任何产品,消费者应该以实际的产品标签内容为准,尤其应关注重要的安全信息以及产品最新信息,包括剂量、使用方法和禁忌症等。
- 由于循证医学研究、文献及有关产品处于不断的变化中,本网站工作人员将尽力更新。
- 本网站不能保证所载文章内容、综合干预方案以及相关成分或产品述及的健康益处,也不承担任何责任。